HEOR Strategy
Too many life science companies arrive at the point of health technology assessment (HTA) submission or payer engagement without a coherent evidence strategy.
Clinical studies may have been designed to satisfy regulators rather than payers, endpoints chosen simply for their clinical convenience and real-world evidence generated without the necessary methodological rigour. The consequences are predictable: weaker submissions, longer timelines and avoidable failures at precisely the moment when success matters most. Strategic evidence generation — the discipline of mapping what evidence will be needed, designing credible studies, filling gaps in the evidence and managing the process over time — is what separates organisations that build compelling evidence packages from those that scramble to assemble whatever they happen to have.
This course provides a structured, end-to-end framework for planning and designing an evidence generation strategy from the earliest stages of the product lifecycle through to HTA submissions and beyond. Over eight modules, participants learn how to map the decision landscape, engage with HTA bodies, conduct gap analyses, plan the sequence of clinical and economic evidence generation and choose appropriate study designs. The result is a costed evidence roadmap that aligns cross-functional teams around a shared strategy and leads to successful downstream submissions.
Delivered via IHLM’s online learning platform and through live interactive virtual tutorials you will become part of a global community that is building compelling evidence for healthcare decision-makers.
On completion of this course you’ll be able to:
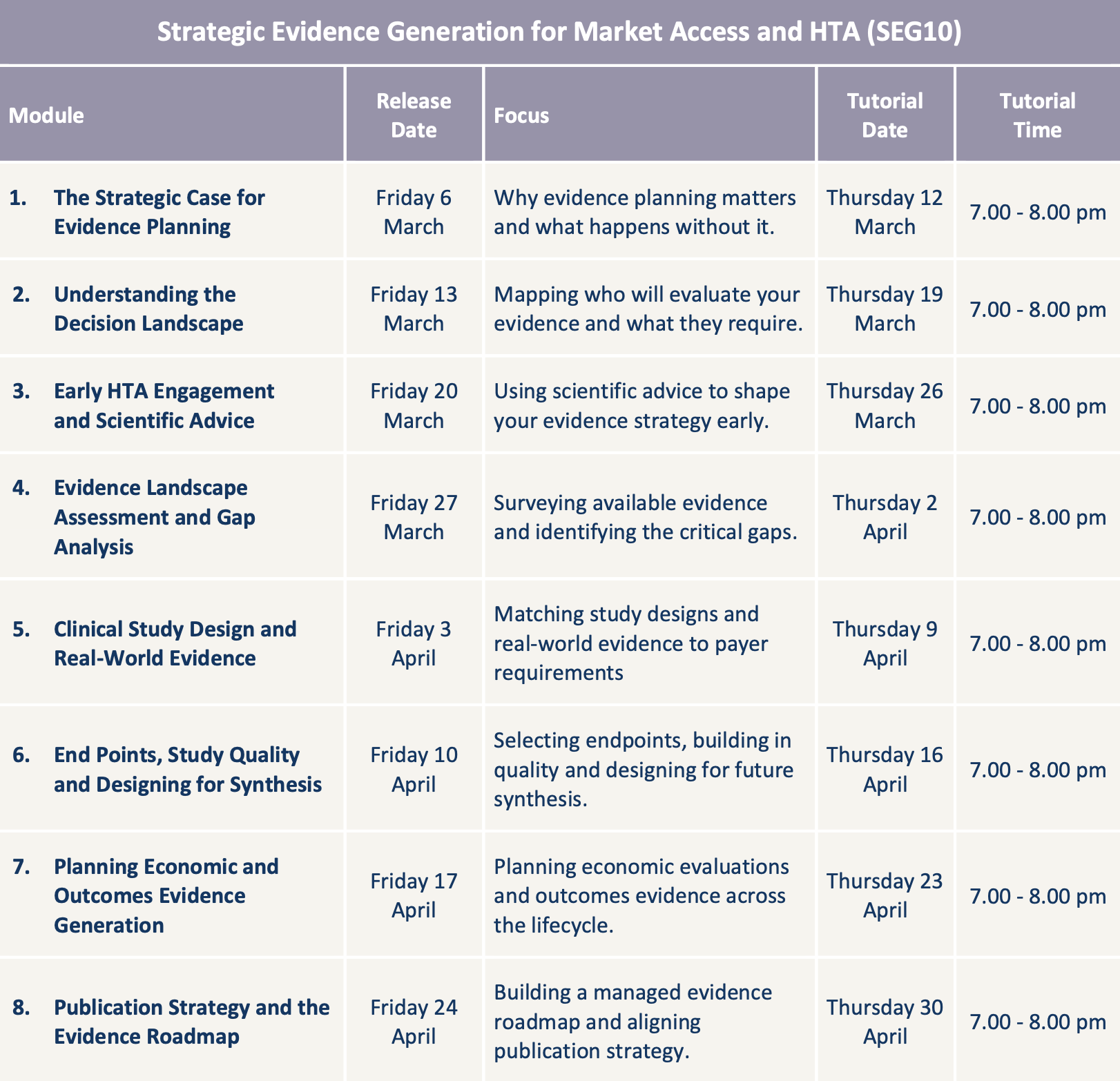
This course is broken down into eight manageable weekly modules:
This course should take approximately 6 – 8 hours per week. You can expect to devote about 2 – 3 hours per week to self-paced learning, about 2 hours per week preparing for and participating in the virtual tutorial and 2 – 3 hours per week applying your knowledge through learning activities and mini-projects. Every tutorial is recorded so you can rewatch it at any time.
This course is designed for market access professionals, medical affairs specialists, HEOR managers and commercial leaders in the life sciences industry who are responsible for planning or overseeing the evidence that supports reimbursement, HTA submissions and procurement decisions. It is equally relevant for regulatory affairs professionals involved in aligning clinical and HTA evidence requirements and for consultants who advise on evidence strategy. No prior experience of health economic modelling or evidence synthesis is required, though participants will benefit from familiarity with HTA processes and the healthcare product lifecycle.
Upon successful completion of the course you’ll receive an:
Ready to start? Just click the ‘Register now’ button at the top of this page or use the ‘Ask us a question’ button if you’d like to talk to one of our course facilitators. The fee for this course is £995 per person. If you’d like to pay in instalments you can arrange this by contacting us at: registration@ihlm.org.
All registrations are subject to our terms and conditions which are available here. By registering for an IHLM course you are accepting these terms and conditions and agreeing to be bound by them.
Many medical device, diagnostics and digital health companies routinely reach the point of seeking reimbursement or the approval of a health technology assessment (HTA) body without a coherent evidence strategy behind them. Our first module makes the case for early, structured evidence planning and explains why reactive, piecemeal approaches to evidence generation lead to weaker submissions, wasted budgets and avoidable delays.
Before any evidence can be planned, the first question is: evidence for whom? This module maps the decision-makers and frameworks that determine whether a product achieves reimbursement, formulary listing or procurement and identifies what each requires in terms of evidence type, quality and format.
One of the most underused tools in evidence planning is the opportunity to ask decision-makers directly what they want to see. This module covers the formal scientific advice and early dialogue processes offered by HTA bodies and regulatory agencies and explains how to use them to shape an evidence strategy before committing resources.
With the decision landscape and any early HTA feedback in hand, the next step is to survey what evidence already exists and measure it against what is required. This module covers how to conduct a structured landscape assessment, catalogue available evidence and systematically identify and prioritise the gaps that the evidence generation plan must address.
With gaps prioritised, the question becomes how to fill them. This module covers the full spectrum of available study designs — from randomised controlled trials through prospective registries to retrospective database studies — and provides a practical framework for selecting the right design based on what payers and HTA bodies will accept.
The endpoints a study measures and the rigour with which it is conducted determine whether its results will survive HTA scrutiny — and whether they can be combined with other studies in a future systematic review or meta-analysis. This module covers the design decisions that are easy to get wrong at protocol stage and impossible to fix afterwards.
Clinical evidence alone rarely secures reimbursement. This module covers when and how to plan for economic evaluations, health-related quality of life data collection and other outcomes evidence that HTA bodies and payers expect — and how to sequence these activities around the product lifecycle.
Evidence that has not been published cannot be cited in a submission, and an evidence plan without governance will not be delivered. This final module brings together publication strategy and operational planning into a single, actionable evidence roadmap — sequenced, costed and managed.

Healthcare Leadership

Our flagship course for high-potential healthcare leaders: built around the core strategic management disciplines and designed to prepare you for more senior roles and greater responsibilities.
Patient Experience

A comprehensive course for progressive healthcare providers and professionals who want to design and deliver more person-centred, compassionate and responsive care.
HEOR Strategy

This course enables you to plan, design and manage the clinical and economic evidence needed to support market access, reimbursement and health technology assessment.
Health Technology Assessment

This course will enable you and your healthcare organisation to achieve operational excellence by improving capacity, productivity and patient flow at every stage of care.
Value Communication

Discover how to set up effective error reporting systems, lead investigations into adverse incidents, implement successful patient safety improvement projects and design safer systems of care.
Value Communication

This course will enable you to master the concepts, methods and tools you need to lead successful quality improvement projects or become a quality improvement specialist.
Health Economic Modelling

A practical, Excel-based course on how to design, build and present budget impact models for health technology assessments, business cases and value propositions.
Health Economic Modelling

This hands-on course shows you how to build, interpret and present cost-effectiveness and cost-utility models that measure the value of health interventions and guide healthcare decision-making.
Evidence Review and Synthesis

Discover how to plan, commission and evaluate rapid evidence reviews that generate accelerated, evidence-based insights in response to time-sensitive demands.
Real-World Evidence

A practical course that equips you to design, conduct, analyse and appraise observational studies that generate credible evidence for HTA bodies and payers.
Evidence Review and Synthesis

A practical course that will enable you to compile, appraise and summarise existing research using the “gold standard” in evidence-based decision-making.
HEOR Strategy

Discover how artificial intelligence is reshaping health economics and outcomes research — and what it means for the professionals who commission and undertake this work.
Value Communication

Discover how to transform clinical, economic and outcomes evidence into a compelling value story that convinces decision-makers and accelerates market access.
Health Technology Assessment

This case study-based course introduces you to the fundamentals of health technology assessment and how to get submissions right first time.
February 13, 2026
Introducing yourself properly is surely a basic necessity if we’re to be a respectful and trusted caregiver?
May 9, 2025
Can glove change help reduce the costs and improve the outcomes of caesarean sections – enabling obstetric teams to deliver more value-based care?
Course starts: 05 March 2026
Location: Online
Course starts: 05 March 2026
Location: Online